
 I am a Board-Certified Orthopedic Surgeon who sub-specializes in spinal surgery. When I came into practice in 2003, my goal was to become a Physician who was completely specialized in spinal surgery only. By 2005, I no longer performed general orthopedic surgery; meaning that I no longer performed hip, knee, shoulder, hand or foot surgery. My practice is completely dedicated to the operative and nonoperative treatment of the cervical, thoracic and lumbar spine. By performing a large volume of spinal procedures, I have the benefit of experience. I believe this experience has helped me avoid complications and determine who surgical intervention will help and who it will not.
I am a Board-Certified Orthopedic Surgeon who sub-specializes in spinal surgery. When I came into practice in 2003, my goal was to become a Physician who was completely specialized in spinal surgery only. By 2005, I no longer performed general orthopedic surgery; meaning that I no longer performed hip, knee, shoulder, hand or foot surgery. My practice is completely dedicated to the operative and nonoperative treatment of the cervical, thoracic and lumbar spine. By performing a large volume of spinal procedures, I have the benefit of experience. I believe this experience has helped me avoid complications and determine who surgical intervention will help and who it will not.
In my practice, we commonly perform lumbar microdiscectomies, lumbar fusions, and cervical fusions. Also, for the past 6 years, I have taken a special interest in cervical disc arthroplasties (cervical disc replacements). I have performed over 700 of these disc replacement procedures.
Like many surgeons, I try to select the most effective and least invasive treatment possible, without increasing risk. When my team and I see a new patient in the office, our number one goal is to diagnose the problem that they have and lay forth a treatment plan. The treatment might be as simple as medication or an order for physical therapy. Other times, a patient will present with a problem that we know will not resolve without surgical intervention. Our goal is to explain these options to the patient, so they can make an educated decision about their treatment plan. If we feel long-term, non-operative pain management and long-term narcotic medications are the best treatment option, there are other specialties that are more appropriate for those patients.
Episodes of low back pain are extremely common and 90% of people will have a major episode of back pain in their lifetime. Most episodes of low back pain resolve on their own, within 6 to 12 weeks. If the patient has lower back pain without any symptoms into the legs, then we believe initial treatment does not require spinal surgery consultation. I would generally recommend that the patient ask their Primary Care Physician, for anti-inflammatory or steroid medication to help calm down the inflammation which leads to many episodes of back pain and to consider physical therapy. It is also important for the patient to understand that even though symptoms can be quite severe at first, it can be surprising how much resolution of symptoms happen on their own within a few weeks to a few months.
In patients that have back pain that continues to trend in a negative direction over several months, is intractable, or is persistent for greater than 3 months, I believe it is reasonable to obtain an MRI to try to reach a more definitive diagnosis. In our practice, we do not have one specific timeline for when it is appropriate to get an MRI, as every patient is different. In some people, they clearly do not require an MRI and others should have it performed much sooner than many guidelines recommend. Our goal is to obtain the appropriate imaging when it makes the most sense for the patient. The most important thing in treating chronic back pain is to first come up with the correct diagnosis, as treatment varies markedly depending on the primary cause. The most common causes of chronic lower back pain are arthritis of the joints, lumbar stenosis, and spinal instabilities like lumbar spondylolisthesis or disc degeneration. It is common to have these problems on an MRI Scan without them being the cause of the patient’s symptoms. Thus, there is need for a thorough evaluation to determine the exact origin of symptoms. Once a diagnosis has been obtained, we are in a much better position to determine if surgery is indicated.
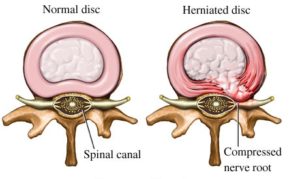
The lumbar disc is basically the cushion that sits between the bones of the lumbar spine, which provides stability and shock absorption. Over time, everybody’s discs degenerate to some degree and this is part of normal aging. A disc is made up of several parts, primarily a tough outer part and the soft inner core. A lumbar disc herniation is when the soft inner part pushes through the tough outer part. When the soft inner disc material pushes through the outer part and lands against a nerve, the patient can develop pain in the distribution of that nerve. Disc herniations can occur at any level in the spine but are most common in the lower lumbar spine. When this occurs, patients will often develop pain in the buttock going down into their legs. Many disc herniations improve without surgical intervention, as the natural history of many disc herniations are to improve on their own. Over time, the body can resorb or wall off the disc material that entered the spinal canal, at which time patient quits being symptomatic from it.
Surgical intervention is considered when a patient has a neurologic deficit from the disc herniation or significant discomfort that is failing to improve with nonoperative measures. Different disc herniations have what I would call different personalities; some are quite mild, and others are extremely severe.
When it comes to surgical intervention, most disc herniations can be treated by a procedure known as a lumbar microdiscectomy. This is an out-patient procedure which has the goal of removing the herniated disc material. If a patient’s primary complaint prior to surgery is pain in the buttock and down the leg, the procedure has a very good success rate for relieving this. If a patient has a disc herniation in the central portion of the disc with a primary complaint of back pain, the results of a microdiscectomy are more variable, as some patients with this type disc herniation have pain coming from their disc herniation and others have it coming from structural damage to the disc itself. A lumbar microdiscectomy will not fix back pain from structural damage to the disc. The results of surgery on this type of disc herniation are best determined through a thorough discussion with a surgeon who knows the history of your disc herniation, the history of your back pain, and has reviewed your MRI images.
Lumbar radiculopathy is a condition in which a patient develops symptoms from compression or inflammation of a nerve root in the lumbar spine. The most common symptoms are pain, numbness or tingling going through the buttock down into the legs. Some patients will present with weakness of varying degrees. The two most common causes of lumbar radiculopathy are lumbar disc herniations and lumbar stenosis. A large percentage of patients with symptoms from a disc herniation improve without surgical intervention, as many disc herniations can resorb over time. This leads to spontaneous improvement of symptoms. Nonoperative treatment is aimed at controlling symptoms while the body tries to heal itself. A lumbar microdiscectomy is performed for cases that are more severe and fail to have a good response to nonoperative care. Patients that have lumbar radiculopathy from lumbar spinal stenosis are less likely to have resolution of their symptoms with nonoperative care. Lumbar stenosis is caused by degenerative changes, which do not have a natural history of resorption. It should be noted that the patient with lumbar stenosis causing lumbar radiculopathy will at times improve without surgical intervention. Patients that have symptoms for more than 3 months on a consistent or worsening basis, are less likely to have long term resolution of their symptoms without surgical intervention.
Lumbar Spinal Stenosis is a narrowing of the canals in the spine where our nerves travel, most often because of degenerative changes. This narrowing is often the result of bone spurs off the back of the disc or growing off the joints in the back of the spine. Stenosis can lead to compression of the nerves. The ligament that lines the inside of the spinal canal can thicken and also lead to spinal stenosis. The symptoms of spinal stenosis can range from pain, numbness, and/or tingling going down the legs, to symptoms of the legs feeling tired after standing or walking for a few moments and relieved by sitting down. Spinal stenosis is extremely common and much of it is not symptomatic or is only symptomatic when flared up. In these cases, oral medications, physical therapy, and/or epidural steroid injections can be quite helpful. Patients who have had symptoms for greater than 3 months or who have worsening symptoms are much more likely to require surgical intervention.

A lumbar degenerative spondylolisthesis is a common condition in which the joints in the back of the spine wear out. This leads to one bone sliding forward on another bone. As this occurs, this leads to narrowing of the nerve tunnels, which can cause pain into the buttock, and possibly into the legs. The condition can present many different ways. Symptoms may consist of mild back pain from the arthritic component, severe pain in the back, severe pain in the legs, or even weakness in the legs. The best way to understand this condition is to think of it as mild, moderate, or severe. In many ways, it is not that different than knee arthritis. People with mild knee arthritis often respond to physical therapy and an injection and do not need a knee replacement. People with severe degeneration of their knee joint that can only walk 100 feet before they have pain are probably not going to get better until they have a complete knee replacement. It is similar in patients with a lumbar degenerative spondylolisthesis. People with early/mild degeneration often respond to physical therapy, weight loss, core conditioning and possibly epidural steroid injections. People with severe erosion of the joints in the back of their spine with significant instability and 3 months of progressively worsening symptoms are very unlikely to have resolution of their symptoms without surgical intervention. The decision for surgery is based on combining the patient’s history, response to previous treatments and what is found on x-rays and advanced imaging studies. Many patients with this condition require a lumbar fusion for resolution of their symptoms. It is one of the more common reasons a lumbar fusion is performed in the United States.

Lumbar spondylosis is a medical term that simply refers to arthritis, or degeneration of the joints in the lumbar spine. As we age, it is common to see arthritic changes in the lumbar spine and many of these are not significantly symptomatic. Some people will develop more severe degeneration of the joints in their lumbar spine with more consistent symptoms and seek treatment. Maintaining an ideal body weight and keeping your core muscles strong is the first line of treatment and if this is not done, the results of almost any other type of treatment will be quite limited. Physical therapy and daily core exercises are of benefit in some patients. For problems above and beyond that, patients will often see pain management physicians for injections. Our office often refers patients to physicians for evaluation for a rhizotomy (radiofrequency ablation). This is a procedure in which a pain management physician can use a thermal probe to ablate the small nerves that go to the joints in the back of the spine, so that the patient no longer feels the pain from those joints. We do not perform this procedure but often make referrals for it.
The vast majority of arthritis in the lumbar spine does not require surgical intervention. If a patient fails all nonoperative measures and has severe degeneration, surgical intervention can be performed in the form of a lumbar fusion. This will remove the arthritic pain generators from the levels that are operated on.
A lumbar strain is an injury to the muscles or tendons of the lumbar spine secondary to a physical overload of the spine. Lumbar strains should improve on their own over 2 to 3 months. We often see patients who were told that they had a lumbar strain, however, they continued to have symptoms that lasted more than 3 months. In that case, we believe that it is less likely that the primary problem is a pulled muscle or tendon, and more likely some sort of structural injury to another part of the spine. Muscles and tendons would have healed within that time period. In a case of back pain in a patient who was previously told that it was simply a lumbar strain, further diagnostics are required to reach a true diagnosis.